
Violent offenders are usually defined by the crimes they commit—that is, violent offenders are offenders who have committed violent crimes—rather than by some inherent characteristic of the person, such as a genetic defect; no such defect or other similar definitive feature has ever been found. Thus, it is appropriate to describe individuals by their behaviors such as an individual with a history of violent offending or some similar descriptor rather than by using labels such as violent offenders that suggest the presence of some inherent personal features.
There is no universally accepted definition of violent crime; many researchers and authors use their own definitions. Generally speaking, however, crimes that cause physical or significant psychological harm to the victim are considered to be violent crime in contrast with property or nonviolent crimes. One could, however, argue that all crime can cause harm or serious harm to others, even the so-called property crimes. To make things even less clear, new categories of crimes continue to be introduced due to technological or other developments. For example, online bullying is a recent addition; there is no physical or even visual contact between the perpetrator and victim, but it is considered a violent offense. A further caveat is that different countries or jurisdictions use different terms or variations of terms to describe the same or similar acts. Thus, the debate of what constitutes violent crime cannot be easily settled.
While there may not be consensus on what constitutes violent crimes, there is universal consensus that criminal violence must be reduced so all can live in a safer society. There are many approaches to reduce criminal violence such as that based on a public health approach to reduce domestic and spousal violence or the use of early interventions to reduce school bullying and youth violence. This entry focuses on one approach, the Violence Reduction Program (VRP), which provides violence reduction forensic treatment to individuals who are at substantial risk to reoffend violently, the so-called violent offenders, although it begins with a discussion on the types of offenses that are generally considered violent and nonviolent crimes
Violent and Nonviolent Offenses
The types of offenses listed in this section are for general reference only and should not be taken as exhaustive or definitive. What is important is to define the terms violence and violent crime when these terms are used to avoid misunderstanding or miscommunication.
Violent crimes generally consist of homicide-related offenses (murder, attempted murder, and manslaughter), kidnapping, arson, forcible confinement, wounding, robbery, terrorism, various assault offenses, and any sexual assault other than noncontact sexual crimes such as exhibitionism and voyeurism.
Nonviolent crimes are all crimes other than violent crimes such as theft and other property-related offenses, breaking and entering and related offenses, fraud and related offense, and noncompliance and related offenses, such as failing to appear and jumping bail.
There are some crimes that are difficult to categorize partly because their classifications as violent or nonviolent depend very much on the seriousness of the offense, for example, many drug offenses, crimes against the state, and driving offenses.
VRP
The VRP was developed by Stephen Wong and Audrey Gordon; it is an evidence-based program that uses cognitive behavioral interventions to treat problem areas that cause or are closely associated with the person’s criminality and violence. The primary objective of the VRP is to reduce recidivism, especially violent recidivism.
Theoretical Foundations
The development of the VRP was guided largely by the work of Don Andrews and James Bonta and their Risk-Need-Responsivity principles formulated to inform correctional assessment and rehabilitation. Briefly, the Risk principle posits that treatment intensity should match individuals’ risk level, higher risk offenders should receive higher intensity treatment than lower risk offenders. The Need principle specifies that problems that influence or are strongly associated with an individual’s criminality and violence (i.e., criminogenic needs) should be targeted in treatment to reduce the likelihood of recidivism. Within the Responsivity principle, general responsivity maintains that cognitive behavioral approaches should be used to promote positive change within a functional working alliance with staff. Specific responsivity suggests that interventions should be adapted to the individual’s motivation, learning style, cognitive capability, and cultural heritage. Treatment programs that adhered to Risk-Need-Responsivity principles in design and delivery have been assessed as being more effective in reducing recidivism than programs that do not.
Risk Assessment and Treatment
In the VRP, risk assessment and treatment are closely integrated. Risk is assessed using the Violence Risk Scale (VRS), a validated violence risk assessment tool also developed by the VRP authors. VRS scores indicate the level of violent risk and can be used to guide the intensity of treatment (Risk principle). The VRS also identifies treatment targets (Need principle), the person’s readiness or motivation for treatment (Responsivity principle), and risk change over time or between pre- and posttreatment.
Program Content and Delivery
The VRP uses cognitive behavioral therapeutic (CBT) approaches to increase participants’ awareness and understanding of how their thoughts, feelings, and behaviors (TFB) are linked to their offending behaviors. Participants are taught relevant skills necessary to modify their problematic and offense-linked TFB patterns. For example, someone who lacks appropriate interpersonal skills, such as conflict resolution, or lacks emotional management skills, can learn appropriate skills and practice them in daily living to reduce the risk of reoffending. Other maladaptive behaviors and cognitions linked to offending behaviors can be identified and adaptive ones acquired. TFB linked to offending, or treatment targets, can be identified with the VRS.
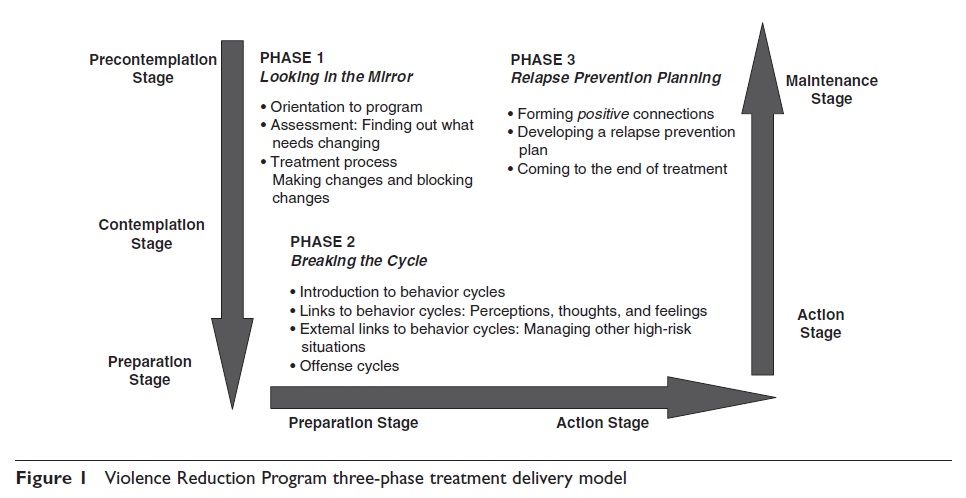
The VRP is delivered based on a three-phase treatment model; learning in one phase is built on learning achieved in earlier phases. Phase 1 or Looking in the Mirror includes VRP modules developed to enhance participants’ understanding of the development and maintenance of offending and violent behaviors, in part, through reflecting on their past and present problems as well as the development of therapeutic alliance and program engagement with staff. The VRS is also used in Phase 1 to identify treatment targets (violence-linked TFBs). The VRP modules within Phase 2 or Breaking the Cycle focus on learning relevant risk-reduction skills using CBT approaches to mitigate treatment targets and TFB patterns identified in Phase 1. By the end of Phase 2, program participants would have developed an offense cycle, which details the personal (dysfunctional TFB) and situational factors linked to their violent offending. Offenders tend to ignore or minimize aspects of their TFB that may be hurtful, incriminating, or likely to evoke guilt or escalate to violence. Thus, participants are encouraged to put together their offense cycles in three separate but related time segments in order to delineate clearly their TFBs prior to, during, and after the offense. Only when they adequately grasp the importance of all relevant TFBs, they can develop comprehensive and effective interventions. Phase 3 or Relapse Prevention represents the consolidation and strengthening of Phase 1 and Phase 2 learning, moving toward the termination of the VRP. In Phase 3, the focus is on the generalization of newly learned behaviors and cognitions acquired in Phase 2 to everyday situations in a custodial setting or, if possible, in the community with appropriate support, encouragement, and monitoring from staff. The application of learning to their everyday environment typically starts in Phase 2 when participants begin to practice taught skills. As a part of Phase 3, participants are required to develop a personal relapse prevention plan linked to their offense cycle. For TFBs identified in each time segment in their offense cycle, participants are required to identify risk-reducing interventions to counter them.
Treatment is a lifelong process of successfully managing one’s behaviors while negotiating and overcoming challenges. Continuity of care is essential to support newly learned skills. Thus, the VRP should be followed by a care plan based on offenders’ individual relapse prevention plan so that participants can be effectively transitioned to their next step in life, whatever that might be, and not left to fend for themselves entirely on their own.
Figure 1 illustrates the VRP three-phase model, the corresponding stages of change, and descriptions of tasks within each phase.
Delivery Format
The VRP is primarily designed as a group-based program. It can also be delivered individually by tailoring the program to those not amenable to group-based programs, such as offenders with learning disabilities or with acute mental health issues.
Program Length
The VRP participants progress in the program by achieving set program objectives rather than by completing a specified number of treatment sessions. Invariably, participants progress at different rates based on personal and situational factors such as their level of risk, need, intellectual abilities, size of treatment group, staffing levels, and other competing priorities. There is an option to incorporate existing treatment modules such as a mandated substance abuse module, in the VRP, which may also affect program length. As a general guidance, for a group of individuals with a significant number of treatment targets (typically medium- to high-risk offenders), the VRP can be delivered in 10–12 months.
VRP Manuals
In addition to the VRS with its own manual for administration, VRP delivery is guided by three program manuals that provide detailed instructions for session, module and phase delivery, and treatment progress evaluations. They are the VRP Facilitator’s Manual, Supplementary Facilitator’s Manual, and the Program Participant’s Manual.
A 24/7 Treatment Model
Within the VRP, a central goal is that participants, with staff support, apply what they learn in group or individual therapy to their daily living— for example, to practice learned skills in interactions with staff and peers, at work, in leisure and recreational activities, in educational or vocational upgradings, 24 hours a day, 7 days a week. In essence, time outside designated treatment hours can be constructively used to extend and consolidate treatment gains. There are many advantages to this approach. Acquired skills are best consolidated by practicing and generalizing them to multiple new situations. Feedback and reinforcements can further shape these behaviors; appropriate prosocial behaviors can be strengthened, and inappropriate behaviors, such as those linked to the individual’s past violence, can be pointed out and addressed swiftly. New skills are best learned if one is immersed in an environment that supports the use of such skills vis-à-vis learning a new language. Line staff who look after the offenders’ day-to-day needs typically spend more time and have more opportunities to observe participants’ behaviors compared to VRP program staff whose observations may be more limited to within formal treatment sessions. Thus, both program and nonprogram staff who have meaningful contact with VRP participants have important roles to play to support VRP program objectives— an extension of the multidisciplinary team concept to include all staff with client contact. Such an approach can also help to engender a supportive change-oriented ethos, thereby fostering an overall positive working environment for all concerned. While the 24/7 treatment approach is not a new concept, few treatment programs have applied it in a custodial setting.
Assessing Treatment Change in Custodial Settings
While changes observed in formal treatment sessions or assessed with self-report questionnaires are important, behavioral observations in participants’ everyday living environment can help to determine the veracity of their behavioral changes. For example, offense-related behaviors easily observable in the community, such as overt aggression, may be repackaged as verbal intimidation or covert bullying behaviors because of close monitoring and severe consequences in prison environments. The prevalence of these repackaged offense analogue behaviors (OABs) is often an indication that the root problems underpinning past antisocial acts have not changed. For each treatment target identified by the VRS, there should be a corresponding and idiosyncratic set of OABs. Change should be evidenced by reduction in OABs across situations with a corresponding increase in appropriate prosocial behaviors or offense reduction behaviors (ORBs) that can be used to successfully manage past problem areas. For example, verbal intimidations and bullying (OABs) should be reduced and replaced by assertive conflict resolution or problem-solving approaches, which are the corresponding ORBs, to deal with real-life challenges.
Assessing the prevalence of OABs and ORBs is critical in determining the presence and consistency of positive (risk reduction) changes in a controlled environment. The VRP’s 24/7 model of treatment provides staff with many opportunities to observe and collect behavioral evidence in support of assessments of change or lack thereof based on the offender’s OABs and ORBs—an evidence-based approach to evaluate treatment progress.
Progress and Treatment Outcome Evaluation
Progress through the VRP is assessed with rating tools provided in the VRP manual for sessions, modules, and for each of the three phases. Progress is based on the participant’s understanding of program material and applying the learning to relevant situations including reducing OABs and increasing ORBs. At the end of treatment or, if necessary, at certain points during treatment, the VRS can be used to assess overall risk changes based on the participant’s progress through the stages of change rubric detailed within the VRS. The overall objective of the VRP is to reduce reoffending in the institution and the community. Treatment progress should lead to overall recidivism reduction, but the latter can only be observed by actual reduction of recidivism in the community and, to some extent, by the reduction of misconduct in the institution.
Treatment outcome results have been examined in a number of studies using different offender groups and research designs. The studies were based either on the VRP or an earlier, but similar, version of the program, the Aggressive Behavioral Control (ABC) program developed in Canada in the mid-1990s. Outcome evaluations of the ABC program allow for much longer follow-up time than VRP-specific studies.
Risk-reduction treatment is sometimes used to reintegrate offenders housed in a very high- security (e.g., super-maximum security) settings to regular high-security settings. Individuals are usually placed in these settings after committing extreme violent acts while incarcerated and their preparation for release to the community often is not the primary objective for intervention. Reported in 2005, 30 offenders from a super-maximum prison in Canada were transferred to the ABC program for treatment in preparation for potential downgrade in security and transfer to a regular high-security prison. The majority (90.3%) were diagnosed with antisocial personality disorder and 80.6% with substance-related disorder. They spent a mean of 6.9 months in treatment. Twenty-five (25) or 83.3% of them were successfully reintegrated into a lower security facility posttreatment without returning to the prison they came from within a 21.3-month follow-up period. Posttreatment institutional offense rates were also lower than pretreatment rates.
In some settings, treatment can be useful to assist extremely disruptive offenders with severe history of violence to better regulate their own behaviors such that they can be managed in the same setting with less restrictive procedures, for example, without the routine use of personal restraints in their movements or the need for constant intensive supervision. Between 2004 and 2006, four prisoners who fit this description, who had committed murder while incarcerated, held in isolation in the highest security prison in England and characterized as extremely difficult to manage, participated as a group in the VRP. In 2006, an independent evaluation of the treatment outcome indicated that participation in the VRP has produced a marked improvement in prisoners’ conduct. Violence-related behaviors had decreased, and interpersonal skills had improved. The authors indicated that, in part, change was due to much improved communications and interpersonal interactions between prisoners and staff thus enabling staff to proactively diffuse high-risk situations prisoners found themselves in. As well, prisoners were better able to manage their emotionally charged reactions. Some limited follow-up information indicated that skills developed during the VRP have since been maintained in less supportive new locations for these prisoners. The qualitative results are consistent with other findings showing violence reduction and behavioral improvement after participation in the VRP, although no firm conclusions could be drawn based on such a small sample size.
Members of various organized gangs, such as motorcycle gangs, and less organized street gangs are particularly challenging for prison authorities to manage and rehabilitate because of their gang affiliation, proneness to peer group pressures, and habitual reliance on violent behaviors. Risk- reduction treatment is an option to reduce their risk of violence but few programs have undertaken systematic evaluation of program efficacy for violence reduction among gang members. Reported in 2006, a group of 40 male treated gang members was compared to 40 untreated or less treated male match controls with a similar demographic profile, including age and race, type of gang affiliation, criminal history, and reoffending risk to ensure that the groups were comparable. Over 78% of the treated group completed the ABC program, the rest attended other CBT risk-focused programs; all were treated for about 7.5 months. In a 2-year follow-up after release to the community, the treated group had significantly fewer and less serious violent and nonviolent recidivism than the controls. After treatment but before release to the community, the treated group also was involved in fewer incidents of major institutional misconduct than the control group. The results suggest that risk-reduction treatment, such as that in the ABC program, is effective in violence reduction even for gang-affiliated male offenders.
Offenders with significant psychopathic personality features are often considered difficult to engage in treatment and are even deemed untreatable by some. As such, risk-reduction treatment of violence-prone offenders with many psychopathic personality features presents major challenges to most treatment programs. In two studies reported in 2012 and 2013, a sample of 150 medium- to high-risk offenders with significant psychopathic features (assessed with the Psychopathy Checklist–Revised) were treated in the ABC program for about 8 months. They were assessed with the VRS to determine their pre- and posttreatment risk levels and to assess changes in risk. The assessments were based on careful reviews of case file information, a well-established and accepted way of data collection for this type of research design. There was a significant reduction in post- compared to pretreatment risk level. In a 5-year follow-up, the risk reduction was found to be linked to the reduction in violent recidivism in the community even after accounting for potential confounds such as level of risk, length of incarceration between treatment termination and community release, and most importantly, the level of psychopathy. The results suggest that risk changes are possible even among high-risk psychopathic offenders. The reduction in risk and recidivism in this offender sample was very likely but not definitively attributable to the effects of treatment, as there was no control group included in this research design.
Another study examined the efficacy of treating high-risk and psychopathic offenders with serious violent criminal histories in the ABC program using a case-matched control group design. Reported in 2012, 32 treated male offenders were matched with 32 male offenders who were either untreated or received some standard routine treatment (treatment-as-usual) within the prison regime. They were matched on violent and nonviolent criminal histories, age, Psychopathy Checklist–Revised scores, and VRS scores and followed up for 7.4 years in the community to determine their recidivism. There were consistent trends of lower violent and nonviolent recidivism in the treated group, but the differences were not statistically significant, probably related to low statistical power due to the small sample sizes. When the seriousness of recidivism was assessed using sentence length as a proxy measure, the treated group showed large, consistent, and statistically significant reduction of offense severity compared to the controls. The results suggest that treatment of a group of high-risk and psychopathic offenders can lead to the reduction of the seriousness of reoffending—a harm reduction effect. The program duration of 8 months for these offenders was likely insufficient to produce an optimal outcome. Despite the less than optimal treatment dosage and having only 32 treated offenders in the group, participation in risk reduction– focused programs, such as the ABC, can reduce reoffending severity. Human costs aside, the offense severity or sentence length reduction alone translated into the equivalent of a net savings of Can$6.2 (approximately US$4.9) million reduction in incarceration costs, as the treated group served significantly shorter sentences than the controls even after factoring in the programming cost. Replications of the study with larger offender samples in different criminal justice settings are essential to provide further support of the present findings.
Final Thoughts
Despite the lack of precision in the definition of violence, the need for reducing violent reoffending, however defined, is universally acknowledged. The VRP, based on Risk-Need-Responsivity principles and CBT approaches, is an empirically tested treatment program designed to reduce violent recidivism and institutional misconduct in forensic clients. Careful program evaluation studies have demonstrated the efficacy of the VRP in the treatment of offenders with psychopathy, housed in super-maximum institutions, and offenders with gang affiliations. That the VRP is effective in reducing reoffending, even in these very challenging offender populations, provides support that the VRP is robust in its design and model of treatment delivery. However, no randomized controlled trial, the gold standard to assess treatment efficacy, has been undertaken on the VRP. The generalization of the evaluation results is limited by the small sample sizes of these outcome studies and by the possible contributions of various moderator variables. More evaluation studies are called for in future research with the VRP.
References:
- Andrews, D. A., & Bonta, J. (2010). The psychology of criminal conduct (5th ed.). Cincinnati, OH: Anderson.
- Di Placido, C., Simon, T., Witte, T., Gu, D., & Wong, S. C. P. (2006). Treatment of gang members can reduce recidivism and institutional misconduct. Law and Human Behavior, 30(1), 93–114.
- Gordon, A., & Wong, S. C. P. (2010). Offense analogue behaviours as indicator of criminogenic need and treatment progress. In M. Daffern, L. Jones, & J. Shine (Eds.), Offence paralleling behaviour: An individualized approach to offender assessment and treatment, (pp. 171–183). Chichester, UK: Wiley-Blackwell.
- Lewis, K., Olver, M., & Wong, S. C. P. (2012). The Violence Risk Scale: Predictive validity and linking changes in risk with violent recidivism in a sample of high risk offenders with psychopathic traits. Assessment, 20(2), 150–164. doi:10.1177/1073191112441242
- Wong, S. C. P., & Gordon, A. (2013). The Violence Reduction Program: A treatment program for violence-prone forensic clients. Psychology, Crime & Law, 19, 461–475. Retrieved from https://doi.org/10.1080/1068316X.2013.758981
- Wong, S. C. P., Gordon, A., & Gu, D. (2007). The assessment and treatment of violence prone forensic persons: An integrated approach. The British Journal of Psychiatry, 190, s66–s74. Retrieved from https:// doi.org/10.1192/bjp.190.5.s66