
The Sex Offender Treatment Intervention and Progress Scale (SOTIPS) is a statistically derived dynamic risk assessment instrument for adult males who have been convicted of sexually abusive behavior. Mental health clinicians, correctional caseworkers, and probation and parole officers use the SOTIPS to assess an individual’s sexual reoffense risk, treatment and supervision needs, and treatment progress. The SOTIPS is designed to be scored at the time an individual begins a treatment or supervision program and thereafter as frequently as every 6 months. The SOTIPS surveys 16 potentially changeable domains (i.e., criminogenic needs or dynamic risk factors) that are related to risk of future sexual offending. The SOTIPS may be used alone or in conjunction with a static sexual offender risk assessment instrument, such as the Static-99R or the Vermont Assessment of Sex Offender Risk-2, which is composed of unchangeable risk factors. When used in conjunction with a static risk instrument, SOTIPS scores can be used to adjust baseline recidivism risk predictions. This article explores the items on the SOTIPS and then explains the criteria for its use, the interpretation of scores, and how to implement this risk assessment tool. SOTIPS Items The 16 SOTIPS items are scored on a scale of 0–3, with higher scores indicating greater treatment need and dynamic risk. Most SOTIPS items are scored to reflect an individual’s cognitive and behavioral functioning for the previous 6 months. SOTIPS items can be clustered into five conceptual categories: sexuality and risk responsibility, criminality, treatment and supervision cooperation, self-management, and social stability and supports. Sexuality and Risk Responsibility The sexuality and risk responsibility category contains 5 items related to sexuality and sexual abuser treatment motivation. The Sexual Offense Responsibility item measures the extent to which an individual internalizes responsibility for his sexual offending behavior. Sexual Behavior measures the proportion of the individual’s non-abusive behavior to offense-supportive sexual behaviors during the previous 6 months. Offense-supportive behavior includes engaging in promiscuous sexual behavior, using pornography in violation of supervision or treatment rules, and engaging in illegal sexual behavior. Sexual attitude addresses the cognitions and beliefs that drive sexually abusive behaviors, including viewing sexual urges as uncontrollable or viewing sexual activity with children as not harmful. Sexual interest quantifies the degree to which the individual’s overall sexual interests focus on offense-related themes, including greater sexual interest in children or rape than interest in consensual sexual activity with consenting adults. Sexual risk management evaluates the individual’s understanding of his risk factors for sexual reoffending and the adequacy of his plan and its implementation to manage his risk in the community. Criminal Behavior The second SOTIPS category contains 2 items that are related to antisocial behaviors and attitudes. Criminal and rule-breaking behavior quantifies behaviors associated with breaking criminal laws, not adhering to probation or parole conditions, or failing to abide by correctional facility rules. Criminal and rule-breaking attitude measures the extent of cognitions and beliefs supporting such behaviors (e.g., “It is only wrong if you get caught” and “Rules are made to be broken”). Treatment and […]
Criminal Justice Research Papers
Sex Offender Risk Appraisal Guide (SORAG)
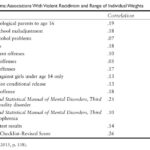
The Sex Offender Risk Appraisal Guide (SORAG) is a 14-item static actuarial risk assessment tool developed to assess risk of general violence (sexual and nonsexual) with adult male sex offenders. After reviewing the development and content of the SORAG, this article discusses its predictive accuracy, strengths, limitations, and applications and concludes with a look at a recent revision merging the SORAG with a companion measure. Development and Item Content The SORAG was developed in 1998 by Vernon Quinsey, Grant Harris, Marnie Rice, and Catherine Cormier at the Mental Health Centre Penetanguishene in Ontario, Canada, a maximum-security psychiatric facility. Although intended to be used with sex offenders, the broad scope of the SORAG is based on the premise that violence as an aggregate outcome is sufficiently serious to merit assessment. For instance, the public is no less deserving of protection from an individual who has committed a nonsexual homicide than an individual who has committed a sexual assault. Furthermore, there is evidence that men who commit sexual offenses (e.g., sexual assault of an adult woman, sexual abuse of a child) have some unique risk factors that set them apart from other violent offenders (e.g., deviant sexual interests, sexual offense history) which are predictive of violence and enough to justify the development of a separate scale. The SORAG was originally developed on 288 adult male sex offenders from four independent samples who were released from Mental Health Centre Penetanguishene and followed up in the community. The rate of violent recidivism observed in the overall sample was 42% over 7 years and 58% over 10 years. The items for the SORAG were identified through statistical procedures aimed at identifying combinations of predictors that optimized the prediction of violence. In all, 14 variables that discriminated violent recidivists from nonrecidivists are listed in Table 1. The correlation for each individual item with binary violent recidivism (i.e., yes–no violently reoffended) is presented in Table 1, along with the weighting of each item. Briefly, correlations are statistics ranging in value from −1.0 to +1.0 representing the strength of association between two variables. When a correlation is computed between one binary variable (i.e., a variable that can take one of only two values, such as inpatient or outpatient or criminally insane or not criminally insane) and another variable with a range of values, this is called a point biserial correlation. Point biserial correlations from .10 to .23 are considered small in magnitude, while those ranging from .24 to .36 are moderate and .37 and above are high. These 14 items were used as the foundation for developing the SORAG. After the best predicting items were identified, a technique known as the Burgess method was used to differentially weight predictor variables shown to successfully discriminate violent recidivists from nonrecidivists. For each category or value of a predictor demonstrating a 5% increase or decrease in recidivism from the overall rate, a weighting of +1 or −1, respectively, is assigned. The weights are increased in either direction based on the degree […]
Self-Report Psychopathy (SRP)
The Self-Report Psychopathy (SRP) scale was designed by Robert D. Hare as a self-report version of his Psychopathy Checklist (PCL) and its revision (PCL-R). Originally created using correctional and forensic populations, the PCL-R is a 20-item construct rating scale that conceptualizes psychopathy as a superordinate dimensional construct composed of four correlated factors: interpersonal (glibness/superficial charm, grandiose sense of self-worth, pathological lying, conning/manipulative), affective (lack of remorse or guilt, shallow affect, callous/lack of empathy, failure to accept responsibility for actions), lifestyle (need for stimulation/proneness to boredom, parasitic lifestyle, lack of realistic long-term goals, impulsivity, irresponsibility), and antisocial (poor behavioral controls, early behavior problems, juvenile delinquency, revocation of conditional release, criminal versatility). Based on a structured interview and file review, PCL-R items are scored on a 0–2 ordinal scale with a recommended diagnostic cutoff score of 30 or above for research and forensic purposes. The PCL-R is considered the international standard for the assessment of psychopathy and helped to significantly advance understanding of the construct by providing a common metric for researchers and clinicians. However, as with any psychiatric interview, the PCL-R requires extensive training and skilled clinicians or researchers to administer it. Thus, the time and cost to train and administer the PCL-R, along with the low prevalence of clinically diagnostic psychopathy in the general population (approximately 1%), lead it to be less practical for non-forensic settings. In addition, certain PCL-R items that are relevant in offender settings (e.g., revocation of conditional release, criminal versatility) may not be appropriate for community samples. For research in the general population, Hare and colleagues developed the SRP. This article focuses on the development and utility of the SRP, as well as its strengths and critique of other psychopathy self-report measures. SRP Development Hare developed the initial versions of both the SRP and the PCL in 1985 after finding that early measures used to assess psychopathy (e.g., Psychopathic Deviate scale from the Minnesota Multiphasic Personality Inventory and the Socialization scale from the California Psychological Inventory) had weak associations with each other and the early PCL. The SRP was developed using standard item reduction procedures to identify items related to psychopathy. Despite developing the initial SRP in the same theoretical framework as the PCL, the agreement between the two instruments was modest. To refine the SRP, Hare and colleagues developed the SRP-II in 1991 to reflect the two-factor structure of the PCL-R. Factor 1 of the PCL-R includes the interpersonal and affective components of psychopathy, and Factor 2 combines lifestyle and antisocial factors. To reflect the PCL-R changes, the SRP-II was expanded to a comprehensive 60-item measure with 31 items specifically designed to capture the two-factor structure. The validity of the SRP-II was bolstered by robust positive correlations with the PCL-R in both clinical and forensic samples. In non-forensic settings, Delroy Paulhus and his colleagues found that SRP-II total scores correlated positively with a variety of antisocial behavioral (e.g., delinquency) and personality (e.g., disagreeableness, promiscuous sexual attitudes) variables. Despite these positive findings, Paulhus and his colleagues […]
Self-Report Measures of Psychopathy
The use of self-report measures to assess psychopathic personality or psychopathy (i.e., a constellation of personality traits and behaviors encompassing guiltlessness, superficial charm, grandiosity, callousness, poor impulse control, and manipulativeness) has been fraught with controversy. Until approximately the 1990s, the overwhelming majority of psychopathy research was conducted in forensic and clinical settings. Since the 1990s, however, interest in studying psychopathic traits in nonclinical settings, such as college and community samples, has burgeoned. Moreover, accumulating research evidence suggests that psychopathy differs in degree rather than kind from normality and is probably underpinned by one or more subdimensions. Given these findings, some researchers have argued that psychopathy can be studied profitably among noncriminal populations by means of self-report measures. Self-report measures have become the predominant mode of psychopathy assessment among nonclinical participants, such as those in college and community samples. This article addresses the potential disadvantages and advantages of self-report psychopathy measures. Criticisms and Potential Disadvantages Self-report psychopathy measures have been met with some criticism. Critics of self-report psychopathy measures point to a variety of features associated with psychopathy, including dishonesty, manipulativeness, grandiose sense of self, and lack of insight, which preclude individuals’ ability to report accurately on their attributes. These criticisms typically reflect skepticism that individuals with extreme psychopathic features are either unwilling or unable to present themselves accurately. This notion is held widely in clinical psychology and psychiatry circles, even among psychopathy researchers. Dishonesty The most obvious characteristics of psychopathy believed to adversely affect the validity of self-reports are dishonesty and manipulativeness. Psychiatrist Hervey Cleckley, who introduced the psychopathy construct to the clinical community in 1941, noted astutely that “the psychopath shows a remarkable disregard for truth.” The lion’s share of research investigating this concern has focused on psychopathy’s relations with response bias, reflecting either a conscious or an unconscious motivation to present oneself inaccurately. Nevertheless, when examined meta-analytically, psychopathy does not relate markedly to various indices of response bias, such as social desirability. In fact, psychopathy is typically negatively associated with underreporting of negative features (i.e., faking good) and positively associated with overreporting of negative features (i.e., faking bad). Contrary to clinical lore, psychopathic individuals are willing to admit to many socially undesirable characteristics and are consistent with higher levels of negative emotionality found in those with chronic antisocial behaviors and impulsivity, which are commonly associated with psychopathy. Lack of Insight A second characteristic of psychopathic individuals thought to adversely affect their self-reports is lack of insight. Cleckley conjectured that psychopathic individuals lack the capacity to see themselves as others see them, calling into question their ability to introspect accurately. Nevertheless, scant research has examined blind spots in psychopathic individuals’ self-perception. It is well established that psychopathic individuals are higher in blame externalization, a trait that is assessed explicitly in certain self-report psychopathy measures. Although there are several potential explanations for this finding, the presence of elevated levels of this trait leaves open the possibility that psychopathic individuals possess little insight into their problematic behavior. Self-Report Versus Informant Report […]
Self-Appraisal Questionnaire (SAQ)
The Self-Appraisal Questionnaire (SAQ) is a theoretically and empirically based instrument. It is the first multidimensional self-administered questionnaire that was specifically designed to predict violent and nonviolent offender recidivism among correctional and forensic populations and to assist with the assignment of these populations to appropriate treatment or correctional programs and different institutional security levels. It was designed to be multifaceted, covering content areas that have been demonstrated to be important for measuring criminogenic factors related to the assessment of recidivism and treatment of offenders. After further describing the SAQ, this article discusses its uses, describes how to score and interpret, and reviews its reliability, validity, and advantages. Description of the SAQ The SAQ was developed in 1996 and published in 2005 with the Mental Health Systems, Toronto. It was designed to cover the predominant predictive areas found in the offender recidivism literature, as some of these areas were ignored or not adequately covered by other tools. The SAQ consists of 72 items, with seven subscales that measure quantitative criminogenic risk/need areas. The first subscale, Criminal Tendencies, taps antisocial attitudes, beliefs, behaviors, and feelings. These tendencies are considered central to the major theories of criminality and the prediction of recidivism. Previous studies, including meta-analysis studies, indicated that the best individual predictors of recidivism were attitudes, values, and behaviors that support a criminal lifestyle. The second SAQ subscale is Antisocial Personality Problems. This subscale covers characteristics similar to those used to diagnose antisocial personality disorder, which has been the psychiatric diagnosis traditionally used to predict recidivism. Self-reported antisocial personality characteristics have been shown to predict static and dynamic factors of violent recidivism. The third subscale, Conduct Problems, assesses childhood behavioral problems. Research has indicated that conduct problems during childhood are among the best predictors of later offending and the development of a criminal career. The fourth subscale considers the offender’s Criminal History, as past criminality has been shown to be a robust predictor of future criminal acts. The fifth subscale is Alcohol/Drug Abuse. The relationship between substance abuse and crime, including violence, is well documented and has been found to correlate with recidivism. The sixth subscale assesses Anti-Social Associates, an area with demonstrated value in the prediction of recidivism. The seventh subscale, Anger, measures the offender’s reaction to anger. This scale is not included in the total score of the SAQ due to the controversial and unconfirmed relationship between anger and recidivism. This subscale could be useful in assigning offenders to anger management or control programs. The Validity scale is a subscale that can be used to validate the offender’s truthfulness in responding to the SAQ’s items. Uses of the SAQ The SAQ can be used for several purposes. First, the SAQ can be used to predict post-release adjustment such as violent and nonviolent recidivism, parole violations, and probability of being convicted of a new offence. The SAQ can also be used to assign offenders to institutional security levels and predict institutional adjustment. Another purpose of the SAQ is the assignment of […]
Screening Assessment for Stalking and Harassment (SASH)
The Screening Assessment for Stalking and Harassment (SASH) is a brief assessment designed to help frontline professionals prioritize stalking and harassment cases for further response. The SASH was developed due to the dearth of frontline assessment tools specifically for stalking, which differs from intimate partner violence in important ways (both the context of the behavior and who it affects). The number and variety of harassment and stalking cases can overwhelm the resources of first responders such as police, victim shelters, and security services. The SASH is designed to help workers in these agencies make informed decisions about prioritization of resources toward cases that are most likely to require additional investigation or management to prevent harm. This article describes the development and structure of the SASH, its use, and empirical findings regarding its reliability and validity. Development of the SASH The SASH was developed by a team of Australian and Swedish clinicians and researchers with expertise in risk assessment of stalking, harassment, and intimate partner violence. Originally called the Stalking Assessment Screen, a 15-item version was developed in 2010 from a review of relevant stalking, violence, and intimate partner violence risk assessment literature. When creating SASH items, the authors also considered the content of three existing structured professional judgment risk assessment instruments that were relevant to stalking: the Stalking Risk Profile (SRP), the Guidelines for Stalking Assessment and Management, and the Brief Spousal Assault Form for the Evaluation of Risk. After reliability and validity trials in Sweden and Australia, the instrument was updated and published as the SASH in 2015. The SASH does not provide a comprehensive assessment of stalking risk. Rather, it aims to accurately identify cases that require no more than a standard frontline response and separate them from cases that may require additional assessment or management to protect the victim. In this way, the SASH can help frontline workers to make evidence-based decisions about prioritizing cases for further attention or referral to specialist services. Using the SASH The SASH is a single-page instrument available in English, Swedish, Dutch, German, and Italian, accompanied by a 20-page user guide. The SASH is designed for use by first responders in stalking situations, such as in general and specialist police teams, domestic violence shelters, security or threat management teams, mental health and forensic mental health agencies, and probation or correctional services. No specialist training or expertise is required to use the SASH, though users are recommended to read the guidelines that provide additional information about rating items and developing responses. The SASH helps to identify cases that are more likely to involve physical violence or prolonged stalking behavior, both of which can be highly damaging to victims. The SASH should be used only in cases where there is evidence of a current pattern of stalking or harassment—that is, a pattern of repeated, unwanted communications or contacts that cause the target apprehension, distress, or fear that occurs outside of an ongoing intimate relationship. The SASH can be used with perpetrators of either sex, […]
Risk Matrix 2000
Of the various approaches used in sexual offender risk assessment (unstructured clinical judgment, actuarial risk assessment instruments [ARAIs], and structured professional judgment), ARAIs outperform all other methodologies. Of the numerous sexual offender ARAIs currently available, the Risk Matrix 2000 (RM2000) is one of the most widely used and researched and is the focus of this article. Description The RM2000 is probably the most frequently used second-generation ARAIs in the United Kingdom. In developing the scale, researchers created a two-dimensional risk assessment system for sex offenders referred to collectively as RM2000. The revised system has two scales, one for measuring risk of sexual recidivism—Risk Matrix 2000/ Sexual (RM2000/S)—and one for measuring risk of nonsexual violent recidivism—Risk Matrix 2000/Violent (RM2000/V) in sexual offenders. The RM2000/S and RM2000/V scales were constructed to yield four summary risk categories: low, medium, high, and very high. The scores of both scales can be combined to give a composite risk of reconviction for sexual or nonsexual assault—Risk Matrix 2000/Combined. In developing the RM2000 scales, the authors referred to a landmark meta-analysis of sexual reoffending predictors as they felt this study offered a more complete guide to the literature, containing more precise and representative estimates of the predictive accuracy of individual factors than would be obtained from any individual study. The RM2000/S uses a two-step system to risk assessment. Step 1 contains three risk items (number of previous sexual appearances, number of criminal appearances, and age divided into three age bands), the sum of which is translated into a risk category. Step 2 considers four aggravating risk factors (any conviction for sexual offense against a male, any conviction for a sexual offense against a stranger, any conviction for a noncontact sex offense, and single–never been married); the presence of two or four aggravating factors raises the risk category by one or two levels, respectively. The RM2000 can only be used if the offender meets the following tests: The offender must be aged 18 years or over. The offender must have at least one conviction for a sexual offense committed when the offender was aged 16 years or over. The offender must be male. All appearances for sexual offenses are counted when scoring RM2000/S, including ones where the offender was under the age of 16 years. The scale can also be used in cases where an individual has been charged with a sexual offense but not yet convicted. The scale has demonstrated good interrater reliability with an absolute agreement for a single rating of 0.90 (which is considered excellent) across 50 cases. The item with the lowest reliability was the noncontact item, which still had good interrater reliability (93.2% agreement). Agreement for the risk category rating is also good (94.9% agreement). Predictive Accuracy Since the 2003 development study, the scale has been independently validated by several research studies using samples in Scotland, Denmark, England and Wales, Canada, and the United States. In the development study, the research group examined the predictive accuracy of the RM2000/S on a treated and […]
Actuarial Risk Assessment
Actuarial risk assessment measures consist of a set of predetermined risk factors (sometimes statistically weighted) that are combined based on an algorithm, which produces a total score that is associated with a final risk estimate or probabilistic statement regarding the likelihood of future recidivism. When assessing risk of general and sexual violence, two commonly used actuarial risk assessment measures are the Violence Risk Appraisal Guide (VRAG) and the Static-99, respectively. Although there has been extensive development and validation of actuarial measures with adult offender populations, there has been limited uptake of purely actuarial measures among young offenders with measures such as the Youth Level of Service/Case Management Inventory representing an adjusted actuarial approach (i.e., lacking in the probabilistic estimate of risk). This article begins by explaining the development of actuarial risk assessment. Next, it describes the strengths and criticisms of actuarial risk assessment. The entry then discusses the use of actuarial risk assessment within a risk management/ treatment paradigm and concludes with a brief discussion of future directions. Development While the initial selection of risk factors for consideration in an actuarial measure can be informed by the broader empirical literature (e.g., meta-analysis), final selection of the risk factors is typically based on their association with an outcome of interest within a development sample (e.g., violent recidivism) and their incremental contribution relative to the other risk factors in predicting outcome. Thus, actuarial measures represent an empirical approach to the risk assessment process. This is not to say, however, that all actuarial measures are void of psychological or behavioral theory. For instance, development of the Level of Service Inventory–Revised, an actuarial risk measure designed for assessing risk of general recidivism, was grounded within the Risk-Need-Responsivity principles and psychology of criminal conduct as developed by psychologist Don Andrews and his colleagues. Strengths of Actuarial Risk Assessment Actuarial risk assessment has consistently outperformed unstructured clinical judgment in predicting short- and long-term violent and sexual recidivism with predictive accuracy that is significantly better than chance. To date, several meta-analytic investigations have found actuarial risk assessment measures to be significant predictors of various forms of outcome such as violence, sexual violence, and general recidivism. Although the majority of the recidivism research has not focused on the nature and severity of violence, there is preliminary evidence to suggest that actuarial measures are significantly associated with such outcomes. This is not surprising, since several of the measure developers have pointed out that actuarial measures were designed to predict these types of outcomes. Unlike clinical judgment, actuarial risk assessment is systematic, impartial, and transparent. Research conducted within applied settings has revealed moderate to high interrater agreement between raters and, in a few instances, between clinicians and researchers (e.g., the Static-99). Likewise, the predictive validity of actuarial risk assessment is similar whether it is scored within an applied (i.e., clinical) or research setting. Similarly, moderate to high predictive accuracy has been found when actuarial measures are scored by frontline staff (e.g., police and parole officers). This highlights an appealing aspect […]
Psychopathy Checklist: Youth Version (PCL:YV)
The Psychopathy Checklist: Youth Version (PCL:YV) is an assessment that measures psychopathic traits and behaviors in youth aged 12–18 years. The construct of psychopathy has been studied in adults with structured assessment measures developed by Robert Hare since the 1970s using the Psychopathy Checklist (PCL), which later became the PCL–Revised (PCL-R), a measure of psychopathy widely used in research, clinical, and forensic settings. The PCL:YV was adapted from the PCL-R and published in 2003. It has the shared goal among researchers and clinicians of identifying psychopathic traits and their consequences in youth, with the potential to shed light on the developmental precursors of adult psychopathy. Furthermore, it provides a means to discover the persistence of these traits from adolescence to adulthood and to assess the effectiveness of early intervention. Adult psychopathy is related to many negative social and individual outcomes, including violent reoffending, instrumental aggression, substance abuse, and treatment dropout. The PCL:YV was constructed to learn the developmental history of psychopathy and its early manifestation with the goal of ameliorating these negative outcomes. This article describes the structure and administration of the PCL:YV, special considerations when assessing adolescents, its psychometric properties, and its application for understanding the construct of psychopathy in youth. Structure and Administration The PCL:YV is a 20-item rating scale completed on the basis of a semi-structured interview and a collateral file review. The rater scores each item on a 3-point scale from 0 to 2, where 2 is definitely present, 1 is somewhat present, and 0 is not present, resulting in a total score ranging from 0 to 40, with higher scores representing more psychopathic traits and behaviors. The file review is typically conducted first to gather and organize information and to help prepare questions for the interview. A rater who typically has an advanced professional or university degree (e.g., MD, MA, PhD) conducts the interview with the youth, which takes approximately 120 minutes. The interview probes different aspects of the youth’s life, including the youth’s history and current functioning, school, work, family background, relationships, substance use, attitudes, emotions, and antisocial behaviors. As a semi-structured interview, its trajectory may change depending on the flow of conversation, cooperation, and types of information shared by the youth. Although not preferable, when an interview is not possible (e.g., youth or parents withhold consent), a PCL:YV assessment can still be conducted with just a file review. File review-only assessments, however, should contain multiple sources of information from varied contexts, should be noted in the assessment report, and its results interpreted cautiously. The PCL:YV manual provides a detailed description of each item for assessors to minimize rater differences when scoring. In addition to detailed descriptions of each item, the manual provides information on where to find the source of information. These are details and illustrations that give the assessor an indication of what information during the interview and/or file review is relevant and helpful for scoring each item. PCL:YV items can be grouped according to factor analysis into four clusters of traits […]
Psychopathy Checklist-Revised (PCL-R)
Robert Hare’s Psychopathy Checklist-Revised (PCL-R) and the briefer screening version (PCL:SV) are the predominant tools for assessing psychopathic traits in adult forensic and correctional settings. Psychopathy is a multidimensional personality disorder characterized by an arrogant and manipulative interpersonal style, poverty in major affective reactions, an impulsive and irresponsible lifestyle, and persistent and inadequately motivated antisocial behavior. Contemporary conceptualizations of psychopathy derive from Hervey Cleckley’s seminal work in the 1940s in which he provided comprehensive descriptions of institutionalized psychiatric case studies. Cleckley defined psychopathy primarily in terms of interpersonal and affective deficits under a surface of outwardly normal behavior, which he termed a mask of sanity. Considerable research has demonstrated that adults presenting with psychopathic traits embark on a chronic, proactively (i.e., without provocation, for instrumental gain) aggressive, violent, and criminal lifestyle, and as such are highly overrepresented in the criminal justice system. The PCL and its derivatives are often used by clinicians and forensic professionals for violence risk assessment, although not originally intended for this purpose. In fact, in his case descriptions, Cleckley did not characterize psychopaths as explosively violent, predatory, or cruel; rather, he suggested that the harm that they caused was secondary to their shallow affect. Modern perception of psychopathy’s association with criminal antisocial behavior stems from William and Joan McCord’s work with incarcerated offenders, rather than psychiatric patients. Many current measures of psychopathy assess law-breaking behaviors in addition to the core affective and interpersonal features, which some scholars view as tangential to the construct, constituting a matter of contention. This is due in part to the fact that most existing measures of psychopathy are based on the PCL, which weighs antisocial and criminal externalizing features as strongly as the traits of emotional detachment and interpersonal exploitation. Research finds that the predictive utility of PCL assessments is largely derived from its assessment of antisocial and disinhibitory tendencies rather than interpersonal and affective features. Psychometric Properties and Factor Structure Hare’s initial efforts toward developing this clinical diagnostic instrument consisted of a global ratings system that was based on Cleckley’s institutional description, in which a diagnostic rating from 1 to 7 was assigned to indicate an individual’s likeness to a prototypical psychopath (1 = clearly nonpsychopathic, 7 = definitely psychopathic). However, this original rating system required considerable experience and knowledge of Cleckley’s conceptualization and was not easy to disseminate to other researchers or clinicians. Hare’s original checklist consisted of 22 items that were chosen from a larger item pool on the basis of how effectively they discriminated, as a set, between high and low scores on the global ratings system. Individuals’ likeness to a prototypical psychopath was rated on a 3-point scale (0 = item does not apply; 1 = item applies somewhat; 2 = item definitely applies). The subsequent revised version (PCL-R) dropped two items (“previous diagnosis of psychopathy or similar” and “antisocial behavior not due to alcohol intoxication”) from the original checklist with poor factor loadings and included clarified scoring criteria for ease of use for evaluators. PCL […]